What is BOAS?
Brachycephalic Obstructive Airway Syndrome refers to a combination of features commonly seen in brachycephalic (short-nosed) breeds, such as Pugs, French Bulldogs, and British Bulldogs. These features include an elongated soft palate and stenotic (narrow) nares which can then lead on to cause secondary changes.
Although not all brachycephalic dogs show clinical signs, there has been an increase in the frequency and severity of the respiratory disorders seen amongst these breeds.
Cats can also be affected by these changes, with Himalayan and Persian breeds most commonly affected.
How does BOAS cause a problem?
Stenotic nares result in reduced airflow through the nose whilst an elongated soft palate can obstruct airflow through the larynx. Tonsils can also become inflamed and enlarged.
The increased air turbulence and negative pressure created by dogs breathing past these obstructions can cause inflammation and swelling of the soft palate, which then partially obstructs the larynx. In addition to this we can also see the start of laryngeal collapse. This typically starts with the laryngeal saccules (pockets of tissue which sit in front of the vocal cords) becoming everted and turning inside out, and can be followed by weakening and collapse of the vocal cords (laryngeal collapse), further obstructing the airway.
If left untreated, these patients are at risk of developing heat stroke, high blood pressure and in some cases heart failure.
Symptoms of BOAS:
- Noisy breathing
- Difficulty breathing
- Snoring
- Exercise intolerance, especially during warm weather
- Collapse
- Excessive panting
- Vomiting or regurgitation
- Poor sleep quality
These signs are usually worse in hot weather and during, or after exercise or excitement. Overweight dogs tend to struggle even more than slim dogs as their airways become even more compressed. In these patients it is essential to instigate a weight loss programme in addition to any corrective surgery.
Regurgitation is commonly seen in dogs with BOAS, as the negative pressure created during breathing results in stomach acid reflux. In some dogs, regurgitation, or bringing up white froth, is often the only clinical sign which is noticed.
Diagnostics:
Stenotic nares can be assessed during the initial clinical examination, whilst the soft palate, larynx and tonsils can only be assessed under a general anaesthetic using a laryngoscope.
A CT scan is performed which allows us to evaluate the head, the lower airways and lungs for conditions such as aspiration pneumonia, hypoplastic trachea (small windpipe) and hiatal hernia.
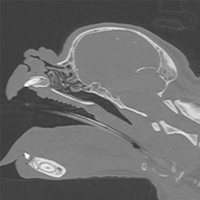
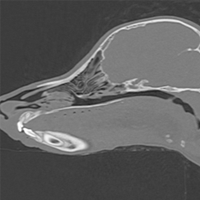
CT scans of a brachycephalic skull compared to a dog with a longer nose.
Surgery:
Corrective surgery is usually performed immediately after our diagnostic investigations.
Surgical widening of the nostrils is performed to improve airflow through the nasal passages.
The soft palate is shortened, and sometimes thinned, to remove excess tissue and therefore create more space at the back of the throat.
If the laryngeal saccules are everted, then these may be removed at the time of surgery. Very large or inflamed tonsils may also be removed at the same time.
Dogs with advanced laryngeal collapse may require further surgery if they do not show sufficient improvement following soft palate shortening and widening of the nares. In these cases we sometimes need to perform a ‘tie-back’ procedure to hold the larynx in a more open position, or we can remove a portion of the laryngeal cartilage to open up the airway. In some advanced cases, our only remaining solution can be to create a permanent opening into the trachea, called a permanent tracheostomy.
Post-operative care
Patients are monitored very closely on recovery from anaesthesia and overnight and are usually discharged the following day.
A small number of patients will suffer with swelling of the tissues at the back of the throat following surgery. These patients will struggle to breathe as the swelling can obstruct the airway. In these patients we will place a temporary tracheostomy tube through an incision in the neck directly into the trachea. These tubes mean that the patient can breathe until a point when the swelling has improved and the patient is able to breathe normally.
Patients will be discharged with oral pain relief. They need to be fed small, soft balls of food little and often for the following two weeks, and exercise kept to a minimum for 7-10 days following surgery.
Whilst BOAS is not a curable condition, corrective airway surgery can provide a much improved quality of life. Young patients with mild signs of respiratory distress tend to respond very well to corrective airway surgery, and we can see a big improvement in their demeanour and ability to exercise following surgery. Whilst we will often see a marked improvement in dogs with previous vomiting or regurgitation in the long term, these clinical signs will often become transiently worse in the first 7-14 days following surgery.
Patients with clinical signs associated with more advanced laryngeal collapse unfortunately carry a less favourable prognosis and may require further surgery.